Perforated peptic ulcer is a common surgical emergency condition worldwide, which is associated with significant morbidity and mortality if early diagnosis and immediate surgical management were not carried out. Perforation occurs in roughly 5% of PUD patients during their lifetime; this study aimed to explore the wide range of clinical presentations, associated risk factors, complications, and surgical management of perforated peptic ulcer patients.
A 5-year retrospective observational study on the clinical presentation and surgical management of perforated peptic ulcer is carried out in a tertiary hospital in Mogadishu, Somalia, Department of General Surgery, from January 2017 to December 2021. We included all patients undergoing operations with an intraoperative confirmed diagnosis of perforated peptic ulcer at the general surgery department. For operated patients, follow-up evaluation was performed in the outpatient department.
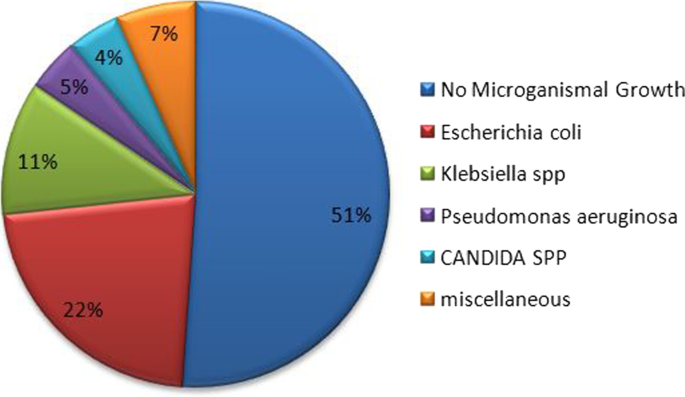
Fifty-one patients underwent an emergency operation for perforated peptic ulcer during the study period. The sociodemographic distribution of patients was 45 (88.2%) males and 6 (11.8%) females, giving a male-to-female ratio of 7.5:1. The mean age of patients was 35.5 ± 16.8 years, and the peak frequency was in the third decade. The commonest presenting symptoms were sudden onset of severe epigastric pain in 42 (82.4%) patients. Patients who presented perforated peptic ulcer within 24 h of initiation of symptoms were free from complications. Age-group and delayed presentation > 48 h after onset of symptoms were linked to postoperative complications and were statistically significant (P 0.032 and P 0.005), respectively. Four patients died (mortality rate of 7.8%). Two patients were reoperated because of the failed primary repair, and 4 patients had > 5 cm intra-abdominal abscess image-guided percutaneous drainage, and the rest were given antibiotic therapy according to peritoneal fluid culture and sensitivity results. The most common microorganism isolated was E. coli 22% and Klebsiella 11%. Other rare microorganisms (pseudomonas, Staphylococcus aureus, and Candida spp.) were identified. In half (51%) of the patients with peritoneal fluid culture, no microorganism growth was seen.
The distribution of perforated peptic ulcer is common in the young age-group in the third decades of life. Delayed presentation of the disease is linked because most patients arrived from remote areas where proper facilities of health care and health education are not available and the patient might come to the hospital in an advanced stage of the disease. We suggest conducting further researches, health awareness related to complications over-the-counter drugs self-medication, and bad habit including smoking, and to improve health-seeking behaviors of society.
Peptic ulcer disease (PUD) affects 4 million people globally each year. The incidence of PUD has been estimated to be between 1.5 and 3%. Perforation occurs in roughly 5% of PUD patients during their lifetime. Perforated peptic ulcer is a common surgical emergency condition worldwide, which is associated with significant morbidity and mortality if early diagnosis and immediate surgical management were not carried out, having a mortality rate that ranges from 1.3 to 20% [1].
PUP is characterized by the classic triad of abrupt abdominal discomfort, tachycardia, and abdominal tenderness. “I hardly believe that anybody can fail in establishing a diagnosis,” Edward Crisp mentioned in 1843 [2].
Young age-group distribution is commonly seen in the developing world, which is mostly predisposed by smoking. With the advanced age in developed countries, these patients tend to be elderly with multiple comorbidities and associated use of NSAIDs, Helicobacter pylori, physiological stress, corticosteroids, and previous history of PUD are risks factors for PUP [3, 4].
According to the diagnostic value of radiological investigation, 75% of patients with perforated peptic ulcer free air under the diaphragm were detected on erect chest/abdominal X-ray.
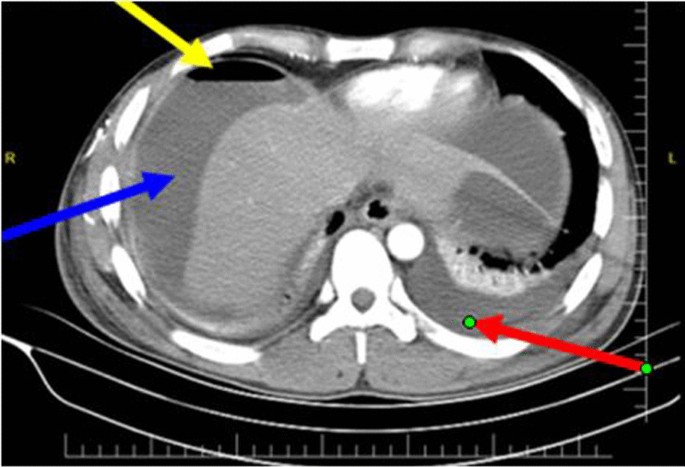
In comparison with a computed tomography scan which reveals superior diagnostic accuracy of 98%, a CT scan can help to distinguish other mimicking differential diagnoses of the acute abdomen like acute pancreatitis that would not require surgical intervention; the utility of this CT scan is justified when the clinical presentation is not specific to upper gastrointestinal pathology or malignancy is suspected and patients’ hemodynamic is not deranged [6].
Exploratory laparotomy and omental patch repair remain the gold standard. Laparoscopic surgery should be preserved in the early presentation of disease and diminished associated complications. Definitive anti-ulcer surgery is significantly associated with fatal outcomes in these patients, while it increases the length of the operation, exposes the patient to prolonged anesthetic time, and increases the chance of postoperative complications. Gastrectomy is recommended in patients with a large or malignant ulcer [7, 8].
The present study aimed to explore the wide range of clinical presentations, associated risk factors, complications, and surgical management among patients with perforated peptic ulcer. There has been no previous research related to this topic in the country, and this research will be a foundational study in the field.
A 5-year retrospective observational study on the clinical presentation and surgical management of perforated peptic ulcer is carried out in a tertiary hospital in Mogadishu, Somalia, Department of General Surgery, from January 2017 to December 2021.
Mogadishu Somali Turkey Recep Tayyip Erdoğan Training and Research Hospital is one of the country's main referral hospitals, located in Mogadishu, the capital city of Somalia. It has a bed capacity of 250, 7 operating rooms, 28 intensive care units, 28 dialysis machines, and 300 dialysis beds, as well as a radiology department with diagnostic facilities (digital X-rays, ultrasounds, CT scanner, 1.5 T MRI, fluoroscopy) capable of performing many interventional procedures, such as ultrasound-guided and CT-guided percutaneous drainages, and serves people seeking health care from all over the country. It is also a teaching and consulting hospital that offers residency programs in 19 different specialties.
The patients were identified and extracted from hospital electronic medical records; 51 patients operated on perforated peptic ulcer for emergency surgery were reviewed, where patient clinical information including patient demographic characteristics, diagnoses, investigative (laboratory and radiological) workup, performed surgical procedure, complications, hospital stay, pathology results, peritoneal fluid culture and sensitivity, and mortality was reviewed.
A comprehensive history and physical examination were performed followed by blood investigations (e.g., CBC, liver and renal function test, electrolytes, viral markers, and blood group). Radiological investigations like X-ray abdomen erect, chest X-ray and, if necessary, an abdominal CT were performed in patients on the suspicion of diagnosis of perforated PUD.
The diagnosis of perforated peptic ulcer was confirmed with laparotomy and simple closure of the perforation by primary closure of the defect by 2.0 vicryl, and then application of the omental flap (modified Graham patch repair/omentopexy) was done.
Intraoperatively, copious saline irrigation was done and all gastric ulcers were taken a biopsy of the border of the ulcer in a systematical manner, and peritoneal fluid samples were taken for culture and sensitivity analysis.
We included all patients undergoing operations with an intraoperative confirmed diagnosis of perforated peptic ulcer at the general surgery department.
Those who operated in another hospital and were later referred to our hospital and those who operated in the pediatric surgery department were excluded from the study.
For operated patients, a 3–6-month follow-up evaluation was performed on an outpatient basis depending on their compliance.
We used the Stata version 15 (StataCorp, College Station, TX) statistical program to perform statistical data analysis. Data were presented in proportions and frequency tables for categorical variables. To summarize the data for continuous variables, we utilized ranges, medians, and inter-quartile ranges (IQRs). We computed P values for categorical variables using the odds ratio (OR) and its 95% confidence interval (CI). We determined the variables associated with the outcome using logistic regression, and to adjust for confounding variables, we used multivariate logistic regression and direct standardization techniques. The significance was defined as a P value of 0.05 or less.
Fifty-one patients underwent an emergency operation for perforated peptic ulcer during the study period. The sociodemographic distribution of patients was 45 (88.2%) males and 6 (11.8%) females, giving a male-to-female ratio of 7.5:1.
According to the age-group of the study population, they ranged from 18 to 70 years, with a mean age of 35.5 ± 16.8 years. The peak frequency was in the third decade (20–30 years).
The most common presenting symptoms were sudden onset of severe epigastric pain in 42 (82.4%), abdominal tenderness in 41 (80.4%), abdominal distention in 36 (70.6%), and vomiting in 31 (60.8), clinical signs of peritonitis were seen in 38 (74.5%), and < 90 mmHg systolic pressure was observed in 15 (29.4%) patients (Table 1).
A hospital stay of the patients ranged from minimum of 4 days to a maximum of 20 days; the mean average admission day was 8.7 ± 3.4 days.
The most common complication seen in these patients is pleural effusion which accounts for 29 (56.9%); the second foremost complication noticed in this study was acute renal failure which is about half (23 (45%)) of the patients. Surgical site infection was noted in nearly one-third (16 (31.4%)) of the patients, three patients (5.9%) developed an incisional hernia after 1 year of primary surgery, and only two patients encountered repair site leak (Table 2).


Despite the fact that perforated peptic ulcer disease is a common surgical emergency and that eradication of Helicobacter pylori has resulted in a vast decline in peptic ulcer prevalence, the number of patients requiring surgery has remained relatively constant [9].
The distribution of perforated peptic ulcer is common in the young age-group in the third decades of life; similar studies in Africa and around the globe demonstrated comparable results [8, 10, 11].
Our study demonstrated a male predominance of perforated peptic ulcer, where the majority of the patients were 45 (88.2%) males, giving a male-to-female ratio of 7.5:1 related to other studies where the male/female ratio ranged in 1.3:1 in Tanzania, 3.3:1 in Nigeria, 6.5:1 in Ethiopia, 4:1 in Singapore, and 6.8:1 in Saudi Arabia, respectively [8, 9, 12,13,14].
This study revealed enormous patients with delayed presentation of the disease; this is linked to most patients arriving from remote areas where proper facilities of health care and health education are not available and the patient might come to the hospital in an advanced stage of the disease; related studies agreed these findings [15, 16].
Adoption of national Essential Package of Health Services (EPHS) to all the regions of the country to have access in emergency care facility, as well as training the care providers for early identification of common signs and symptoms of abdominal emergencies, might promote preventing the late presentation of the disease.
The mean average of hospital admission days was 8.7. Long-term hospital stay was discovered as long as 20 days which correlates with late presentation of cases superimposed by consequence complications related to perforated peptic ulcer.
The comparable outcome was documented in various studies in the region and around the globe, concluding that hospital stay and related complications of PUP including death increased in delayed (> 24 h) presentation of the disease [17,18,19].
Positive previous history of peptic dyspepsia was observed in nearly half (25 (49%)) of the patients with peptic ulcer, this might explain the inaccessibility of good health facilities, and most of them may encounter non-professional health workers and traditional healers in many parts of the regions, and patient will seek proper health care facility when condition gets worse and patient develops severe abdominal pain and peritonism. This finding is common in developing countries as several reports stated [8, 10, 13].
The two most common microorganisms isolated were E. coli 22% and Klebsiella 11%; a comparable result was found in a study done in India [20].
Patients with age less than 40 years and delayed presentation of disease were found positive predictors of complications with statistically significant according to bivariate and multivariate logistic regression analyses with a p value of 0.032 and 0.005, respectively. Both factors observed a positive association with postoperative complications. This is particularly noteworthy in developing countries, including Africa, where patients often present late with severe generalized peritonitis, which correlates with a similar study in Tanzania and other parts of the world [8, 21].
The patient with a perforated peptic ulcer and sepsis should be evaluated and identified as early as possible to avoid subsequent organ failure and death [1].
There was no significant association between complications and other above-examined factors.
The mortality rate of 7.8% of patients with perforated peptic ulcer was shown in our study; this substantial rate was worldwide reported in numerous studies as 15.5, 14%, 16.7%, and 27% [19, 22,23,24].
This study has some limitations since it is a retrospective cross-sectional study with a single-center-based design. That might limit the generalizability of the findings.
Perforated peptic ulcer is still a common surgical emergency problem in our country predominantly affecting young males and is associated with substantial morbidity and mortality in delayed disease presentation. Early diagnosis, immediate resuscitation, and urgent surgical intervention are warranted.
Simple primary repair with application omental flap (modified Graham patch repair) is the most appropriate and effective surgical approach in the management of perforated peptic ulcer.
It increases the length of the operation, exposes the patient to prolonged anesthetic time, and increases the chance of postoperative complications.
This is particularly noteworthy in developing countries, including Africa, where patients often present late with severe generalized peritonitis.
Implementation of endoscopic assessment in chronic and intractable dyspepsia will improve the early detection and management of non-complicated peptic ulcer disease.
We suggest further research, preferable to a multicenter study, to determine the epidemiology, associated risk factors, and prognostic factors of the disease in our context, and to conduct health awareness related to complications over-the-counter drugs self-medication and bad habit including smoking and to improve health-seeking behaviors of society.
The data that support the findings of this study are available in Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital information system. Data are, however, allowed to the authors upon reasonable request and with permission of the education and research committee.
Peptic ulcer disease
Peptic ulcer perforation